 |
A returning traveler with two weeks of fever |
- History of Present Illness
- A sailor in his 30s with no significant medical history was admitted to hospital with an 8.2 cm hepatic abscess within the right lobe of the liver. Symptoms started two weeks prior to presentation with fevers, chills and night sweats that progressed to right-upper abdominal quadrant pain. The patient had no headache, neck stiffness, chest pain, shortness of breath, diarrhea, hematochezia, dysuria, extremity swelling or rashes.
- Past Medical History
- No significant medical history.
- Medications
- None
- Epidemiological History
- The patient was born and lived in Nepal until he was a young adult. He immigrated to the United States (U.S.) and lived in the northeast until joining military in his late 20s. His only subsequent travel outside the U.S. was to South Asia a few years prior for one month, and then more recently to the island of Diego Garcia in the Indian Ocean for a military deployment. He had just returned to the U.S. several weeks prior to the onset of symptoms above. He reported multiple stops in Asia on his return trip but noted staying only in hotels. He did report adventurous eating.
- Physical Examination
- He had fever (38.1°C) and tachycardia (106 beats-per-minute) with otherwise normal vital signs and exam notable for abdominal distention and right upper abdomen pain with palpation. No other exam abnormalities were identified.
- Studies
- Initial lab work revealed leukocytosis of 13.6 x103 white blood cells/µL (85% neutrophils, 10% lymphocytes, <1% eosinophils), aspartate transaminase 56 U/L, alanine aminotransferase 60 U/L, alkaline phosphatase 356 U/L and total bilirubin 0.74 mg/dL. Computed Tomography scan of the abdomen with contrast revealed the hepatic abscess (Figure 1).
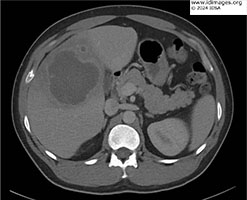 - Figure 1a: Axial image of Computed Tomography of the abdomen with contrast demonstrating an 8.2 cm abscess in the right lobe of the liver.

 - Figure 1b: Coronal images of Computed Tomography of the abdomen with contrast demonstrating an 8.2 cm abscess in the right lobe of the liver.
- Clinical Course Prior to Diagnosis
- See above.
- Diagnostic Procedure(s) and Result(s)
Initial infectious work-up included blood cultures, hepatic abscess cultures (bacterial and fungal), amebiasis antibodies, and echinococcal antibodies. Hepatic abscess fluid was obtained by Interventional Radiology who placed a drain in the abscess with 25 mL of fluid output (Figure 2). Subsequently, a stool culture and stool multiplex GI PCR panel was ordered, the latter of which returned with a positive result for Entamoeba histolytica. At this point the patient’s abscess fluid was separately run on the same assay, which also was positive for E. histolytica.
 - Figure 2: Fluid obtained after drain placement with Interventional Radiology demonstrating red-brown fluid with typical "anchovy paste" appearance.
- Treatment and Followup
- The patient was started on ceftriaxone and metronidazole on admission. After identification of E. histolytica via multiplex GI PCR panel, and with no growth noted on any bacterial culture, the patient was transitioned to monotherapy with metronidazole for 10 days followed by one week of paromomycin for luminal clearance. The patient demonstrated excellent recovery with no recurrence of any symptoms at three months post-treatment.
- Discussion
Hepatic abscesses can be severe and life-threatening infections and the ability to differentiate between bacterial, fungal, and parasitic etiologies quickly is vital to appropriate management. This patient presented for care in an E. histolytica non-endemic region with hepatic abscess and plausible exposure history for E. histolytica. His parasite was rapidly identified by stool test with a multiplex GI PCR panel leading to early changes to his treatment regimen with excellent outcome. While stool PCR has frequently been used to diagnose acute gastrointestinal illness from E. histolytica (3), the use of stool multiplex PCR testing to diagnose amebic liver abscess (ALA) is not clearly established. It is well-established that only 15-35% of patients with ALA have concurrent gastrointestinal symptoms or amebic colitis (4), and as a result older diagnostics like stool microscopy and stool antigen detection are thought to be less helpful for diagnosis of ALA (5). An apparent gap in the literature, however, is data describing the concurrent rate of luminal amebiasis in patients with ALA. Presumably, patients with sequelae of disseminated E. histolytica infection like ALA should still have concurrent luminal infection, whether symptomatic or not. It could then be reasonably extrapolated that in regions non-endemic for E. histolytica the identification of luminal infection in a patient with undifferentiated hepatic abscess would be strongly predictive of ALA.
In recent decades, stool PCR has become the gold standard for diagnosis of intestinal amebiasis with general sensitivity greater than 90% and specificity approaching 100% (1,6). Molecular testing has additional advantages of rapid turn-around time and ability to combine multiple targets into a single assay. In the case above the BioFire® FilmArray® GI Panel was used for diagnosis. This multiplex PCR panel was initially approved in 2014 with 22 separate targets including 4 parasites (Cryptosporidium, Cyclospora cayetanensis, Entamoeba histolytica, and Giardia lamblia) (7). Regarding E. histolytica specifically, this assay has been shown to be 100% sensitive and 89-100% specific for detection of the parasite in stool. This is comparable to other currently FDA approved multiplex PCR panels like the BD MAX® Enteric Parasite Panel and the Luminex xTAG® GI Pathogen Panel, which also can test for E. histolytica (6).
Another consideration in cases like the one presented is potential utilization of multiplex GI PCR panels to test abscess fluid from an undifferentiated hepatic abscess that has been drained or aspirated. Multiple case reports (2,8) have reported successful identification of E. histolytica by testing liver abscess fluid on multiplex PCR panels that otherwise are designed for stool analysis, leading to rapid adjustment of therapy with good outcomes. Other studies have examined non-multiplex PCR in assessing liver abscess fluid. Othman et al reported positive real-time PCR detection of E. histolytica for 23 of 30 liver abscess fluid samples, with 6 of the 7 negative samples having positive bacterial cultures, indicating both high sensitivity and specificity of real-time PCR for this purpose (9). Ghelfenstein-Ferreira et al examined 12 liver abscess samples for E. histolytica with quantitative PCR noting a positive test for all five ALA patients and a negative test for all seven non-ALA patient (10). While multiplex PCR panels are not generally FDA-approved for testing liver abscess fluid, there are relatively clear data that in certain clinical circumstances this type of analysis can have a meaningful and positive impact on infection management.
In E. histolytica non-endemic regions the likelihood of incidental luminal amebiasis is low, so identification of the parasite by stool PCR on a multiplex GI PCR panel in the setting of an undifferentiated hepatic abscess should be highly predictive of ALA. If stool PCR testing for E. histolytica is available, then a practical approach could include two components. First, in patients with undifferentiated hepatic abscess and a plausible exposure history for E. histolytica for whom abscess fluid can be obtained we would recommend consideration of testing the fluid on a multiplex GI PCR panel. Alternatively, in patients with undifferentiated hepatic abscess and a plausible exposure history for E. histolytica in whom obtaining abscess fluid is not possible (abscess too small or in a high-risk location for drainage), we would recommend consideration of testing stool on a multiplex GI PCR panel. The positive and negative predictive value of this testing strategy should provide rapid and useful information to assist with management decisions.
- Final Diagnosis
- Amebic Liver Abscess
- References
-
- Shirley DA, Farr L, Watanabe, K et al. A Review of the Global Burden, New Diagnostics, and Current Therapeutics for Amebiasis. Open Forum Infectious Diseases. 2018. 5(7). doi: 10.1093/ofid/ofy161.
PMID:30046644 (PubMed abstract)
- Weitzel T, Cabrera J, Rosas R, et al. Enteric Multiplex PCR Panels: A New Diagnostics Tool for Amoebic Liver Abscess? New Microbes and New Infectious. 2017. 15(18): 50-53. doi: 10.1016/j.nmni.2017.05.002.
PMID:28626584 (PubMed abstract)
- Roy S, Kabir M, Mondal D, et al. Real-Time PCR Assay for Diagnosis of Entamoeba Histolytica Infection. Journal of Clinical Microbiology. 2005. 43(5): 2168-2172. doi: 10.1128/JCM.43.5.2168-2172.2005.
PMID:15872237 (PubMed abstract)
- Sifri CD, Madoff LC. Infectious of the Liver and Biliary System (Liver Abscess, Cholangitis, Cholecystitis). Mandell, Douglas, and Bennett’s Principles and Practices of Infectious Diseases, Ninth Edition. 2020. 1037-1045.
- Hague R, Mollah NU, Ali I, et al. Diagnosis of Amebic Liver Abscess and Intestinal Infection with the TechLab Entamoeba histolytica II Antigen Detection and Antibody Tests. 2000. Journal of Clinical Microbiology. 38(9) 3235-3239. doi: 10.1128/JCM.38.9.3235-3239.2000.
PMID:10970364 (PubMed abstract)
- Ryan E, Paparini A, Oskam C. New Technologies for Detection of Enteric Parasites. Trends in Parasitology. 2017. 33(7): 532-546. doi: 10.1016/j.pt.2017.03.005.
PMID:28385423 (PubMed abstract)
- Binnicker MJ. Multiplex Molecular Panels for Diagnosis of Gastrointestinal Infection: Performance, Result Interpretation, and Cost-Effectiveness. Journal of Clinical Microbiology. 2015. 53(12): 3723-3728. doi: 10.1128/JCM.02103-15.
PMID:26311866 (PubMed abstract)
- Portunato F, Bartalucci C, Vena A, et al. Amoebic Liver Abscess: Potential Application of New Diagnostic Techniques for an Old Pathogen. Infectious Diseases and Therapy. 2024. 13(3): 625-632. doi: 10.1007/s40121-024-00934-1
PMID:38459236 (PubMed abstract)
- Othman N, Mohamed Z, Verweij, et al. Application of Real-Time Polymerase Chain Reaction in Detection of Entamoeba histolytica in Pus Aspirates of Liver Abscess Patients. Foodborne Pathogens and Disease. 2010. 7(6): 637-641. doi: 10.1089/fpd.2009.0427.
PMID:20132028 (PubMed abstract)
- Ghelfenstein-Ferreira T, Gits-Muselli M, Delliere S, et al. Entamoeba histolytica DNA Detection in Serum from Patients with Suspected Amoebic Liver Abscess. Journal of Clinical Microbiology. 2020. 58(10). doi: 10.1128/JCM.01153-20.
PMID:32759355 (PubMed abstract)
- Notes
ID Week 2024 - Fellows' Day
LCDR Jeffrey Spiro, MD - Naval Medical Center San Diego
- Citation
- If you refer to this case in a publication, presentation, or teaching resource, we recommend you use the following citation, in addition to citing all specific contributors noted in the case:
Case #24006: A returning traveler with two weeks of fever [Internet]. Partners Infectious Disease Images. Available from: http://www.idimages.org/idreview/case/caseid=617
- Other Resources
-
Healthcare professionals are advised to seek other sources of medical information in addition to this site when making individual patient care decisions, as this site is unable to provide information which can fully address the medical issues of all individuals.
|
|