- Diagnostic Procedure(s) and Result(s)
EGD (esophagogastroduodenoscopy)
-
Small bowel, duodenum, biopsy: Acute duodenitis with Strongyloides organisms. CMV, HSV and adenovirus immunohistochemistry negative (Figure 3)
-
Stomach, antrum, biopsy: Positive for Strongyloides organisms. Portions of oxyntic and antral type gastric mucosa with chronic inactive gastritis. Negative for Helicobacter pylori organisms on routine staining. Negative for intestinal metaplasia or dysplasia
Skin abdomen punch biopsy (Figure 2)
-
Orthokeratosis overlying an essentially unremarkable epidermis. Within the superficial and deep dermis, there is a mildly dense perivascular lymphohistiocytic infiltrate with numerous admixed eosinophils. Additionally, there are basophilic exogenous structures, consistent with nematode larvae, percolating between collagen bundles within the dermis and subcutaneous tissues.
Bronchoscopy with BAL (bronchoalveolar lavage):
-
Cell count and differential: 13,350 RBCs, 48 nucleated cells with 33% neutrophils, 19% lymphocytes, 5% monocytes, 37% macrophages and 6% eosinophils.
-
BAL O&P: rare Strongyloides stercoralis
Lumbar puncture:
-
Cell count and differential: 9 RBCs, 3 nucleated cells (7% neutrophils, 92% lymphocytes, 1% monocytes)
-
Protein 41, glucose 169
-
Bacterial Culture: Vancomycin resistant Enterococcus faecium
Right ventricle, endomyocardial biopsy:
-
Foci of interstitial mononuclear cell infiltrates with numerous eosinophils. There is one biopsy fragment with a granuloma containing an elongated wrinkled eosinophilic structure with numerous faint blue nuclei. In the setting of disseminated Strongyloides infestation, the morphology of this structure is consistent with a degenerated Strongyloides larva.
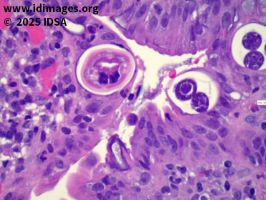
- Figure 3. Small bowel, duodenum, biopsy. Acute duodenitis with strongyloides organisms.


- Figure 6. Stool Ova & Parasite test
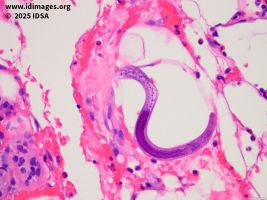
- Figure 2. Skin, abdomen punch biopsy
- Figure 4. CT Chest
- Treatment and Followup
Strongyloides was identified on duodenal biopsy, prompting immediate initiation of oral ivermectin. Because pre-transplant screening of the patient for Strongyloides IgG was negative, there was concern for donor-derived infection which was later confirmed in another recipient from the same donor. A stool O&P confirmed presence of Strongyloides.
Prednisone dosing was reduced and ESBL Enterobacter cloacae bacteremia was treated with meropenem. Despite initial therapy, the patient’s condition worsened, requiring intensive care unit admission for respiratory failure and intubation. Bronchoscopy with BAL demonstrated diffuse alveolar hemorrhage (DAH) and O&P of BAL fluid confirmed presence of Strongyloides larvae, leading to the diagnosis of hyperinfection syndrome. Due to persistent encephalopathy, a lumbar puncture was obtained, with E. faecium on culture which was treated with linezolid.
The abdominal maculopapular rash noted on admission became progressively more purpuric and spread to involve her periumbilical region, bilateral flanks and bilateral proximal anterior thighs (Figure 1). Dermatology was consulted due to high suspicion of cutaneous strongyloidiasis. A punch skin biopsy was obtained and histological examination showed basophilic exogenous structures, consistent with nematode larvae, percolating between collagen bundles within the dermis and subcutaneous tissues (Figure 2).
Patient was initiated on oral ivermectin 200 mcg/kg/day the same day that the EGD results were reported. Due to the development of ileus with concern for impaired enteric absorption, an Investigational New Drug (IND) application was submitted and approved by the FDA for subcutaneous administration of a veterinary preparation of ivermectin, which was started on hospital day 9, at which point her PO ivermectin was discontinued. She finished a course of meropenem for ESBL Enterobacter bacteremia. Stool O&Ps were performed every 3 days while on subcutaneously administered ivermectin. O&P became negative after 12 days of ivermectin (9 days of subcutaneous ivermectin) and she was transitioned back to oral ivermectin once bowel function returned.
- Discussion
This case highlights the potential for donor-derived Strongyloides infection in heart transplant recipients, underscoring the need for vigilant screening in high-risk populations. Early recognition and treatment with ivermectin are critical in preventing progression to hyperinfection syndrome.
Additionally, this case demonstrates both disseminated disease in which there is spread of organism to organs outside of the normal life cycle as well as hyperinfection syndrome, characterized by an accelerated autoinfection.
Treatment challenges exist and include ileus or poor gastrointestinal absorption of ivermectin. In this case, it prompted an IND application for subcutaneous administration of ivermectin.
Cutaneous manifestation of disseminated strongyloidiasis are rare, but periumbilical purpura resembling thumbprints can be a pathognomonic physical exam finding to aid in early diagnosis.
- Final Diagnosis
- Donor-derived Strongyloidiasis Hyperinfection Syndrome with cutaneous involvement.
- References
-
- Kalb RE, Grossman ME. Periumbilical purpura in disseminated strongyloidiasis. JAMA. 1986 Sep 5;256(9):1170-1. PMID: 3735652.
PMID:3735652 (PubMed abstract)
- Periumbilical thumbprint parasitic purpura: A highly fatal sign in disseminated Strongyloides infection that may mimic vasculitis clinically. Journal of the American Academy of Dermatology, Volume 72, Issue 5, AB129
- Pivoto João GA, Alves Antunes IF, Mendes Dos Santos L. Fatal Disseminated Strongyloidiasis with Periumbilical Purpura. Am J Trop Med Hyg. 2021 Jun 28;105(4):860-861. doi: 10.4269/ajtmh.21-0464. PMID: 34181569; PMCID: PMC8592155.
PMID:34181569 (PubMed abstract)
- Purvis RS, Beightler EL, Diven DG, Sanchez RL, Tyring SK. Strongyloides hyperinfection presenting with petechiae and purpura. Int J Dermatol. 1992 Mar;31(3):169-71. doi: 10.1111/j.1365-4362.1992.tb03925.x. PMID: 1568809.
PMID:1568809 (PubMed abstract)
- Salluh JI, Bozza FA, Pinto TS, Toscano L, Weller PF, Soares M. Cutaneous periumbilical purpura in disseminated strongyloidiasis in cancer patients: a pathognomonic feature of potentially lethal disease? Braz J Infect Dis. 2005 Oct;9(5):419-24. doi: 10.1590/s1413-86702005000500010. Epub 2006 Jan 6. PMID: 16410894.
PMID:16410894 (PubMed abstract)
- van Hattem S, Schuttelaar ML. Disseminated strongyloidiasis caused by heart donor-to-host transmission presenting with purpura. Clin Exp Dermatol. 2010 Jun;35(4):e149-50. doi: 10.1111/j.1365-2230.2009.03740.x. Epub 2009 Nov 3. PMID: 19886957
PMID:19886957 (PubMed abstract)
- Weiser JA, Scully BE, Bulman WA, Husain S, Grossman ME. Periumbilical parasitic thumbprint purpura: strongyloides hyperinfection syndrome acquired from a cadaveric renal transplant. Transpl Infect Dis. 2011 Feb;13(1):58-62. doi: 10.1111/j.1399-3062.2010.00516.x. PMID: 20525017.
PMID:20525017 (PubMed abstract)
- Zeitler K, Jariwala R, Restrepo-Jaramillo R, Kapadia S, Casanas B, Alrabaa S, Sriaroon C. Successful use of subcutaneous ivermectin for the treatment of Strongyloides stercoralis hyperinfection in the setting of small bowel obstruction and paralytic ileus in the immunocompromised population. BMJ Case Rep. 2018 Jun 4;2018:bcr2017223138. doi: 10.1136/bcr-2017-223138. PMID: 29866667; PMCID: PMC5990086.
PMID:29866667 (PubMed abstract)
- Notes
IDWeek 2025- Fellows’ Day
Ana Khazan, MD, MPH – Cleveland Clinic Foundation
Contributors: Dr. Chroistopher Kovacs, Dr. Amanda Vest, Dr. Mohamed El Hag, Dr. Martan Rothschild, Dr. Omar Mehkri, Andrea Pallota PharmD
- Citation
- If you refer to this case in a publication, presentation, or teaching resource, we recommend you use the following citation, in addition to citing all specific contributors noted in the case:
Case #25001: When the Past Resurfaces: An Infectious Complication After Heart Transplant
[Internet]. Partners Infectious Disease Images. Available from: http://www.idimages.org/idreview/case/caseid=620.
Please also add copyright information, either “Copyright Partners Healthcare System, Inc. All rights reserved,” or, if provided with the case, other specific copyright information that is followed by “All rights reserved”.
- Other Resources
-